This bronchiolitis season is going to be different. While SARS-CoV2 virus does not seem to be a significant cause of wheeze in children (1), all the other usual viruses are still out there and will be causing wheeze soon in a child near you. What might have changed is how we make decisions about that child.
For the purposes of exploring our decision making, it is important to define bronchiolitis as a condition that is a virally induced inflammation of the small airways of the lungs in a child, typically under the age of 1. It is clinically distinctive from viral induced wheeze which is virally induced bronchospasm of the large airways, typically in a child over the age of 1. For a separate article on differentiating these two conditions, click this link.
The necessary decisions regarding bronchiolitis haven't changed. What might change during a global pandemic is the outcome of those decisions. Hospitals have always been dangerous places, with a significant risk of hospital acquired infection. That risk has escalated due to the prevalence of the highly infective SARS-CoV2 virus. Though very unlikely to cause COVID-19 infection in children, there is that risk, the risk of PIMS-TS and the risk of COVID-19 to the accompanying adults.
The aim in bronchiolitis decision making has always been to keep as many children out of hospital as is safe to do so. In order to do that expertly, we just need to make three decisions.
- Does this child have bronchiolitis?
- Should this child be managed at home or in hospital?
- What treatment should the child be given?
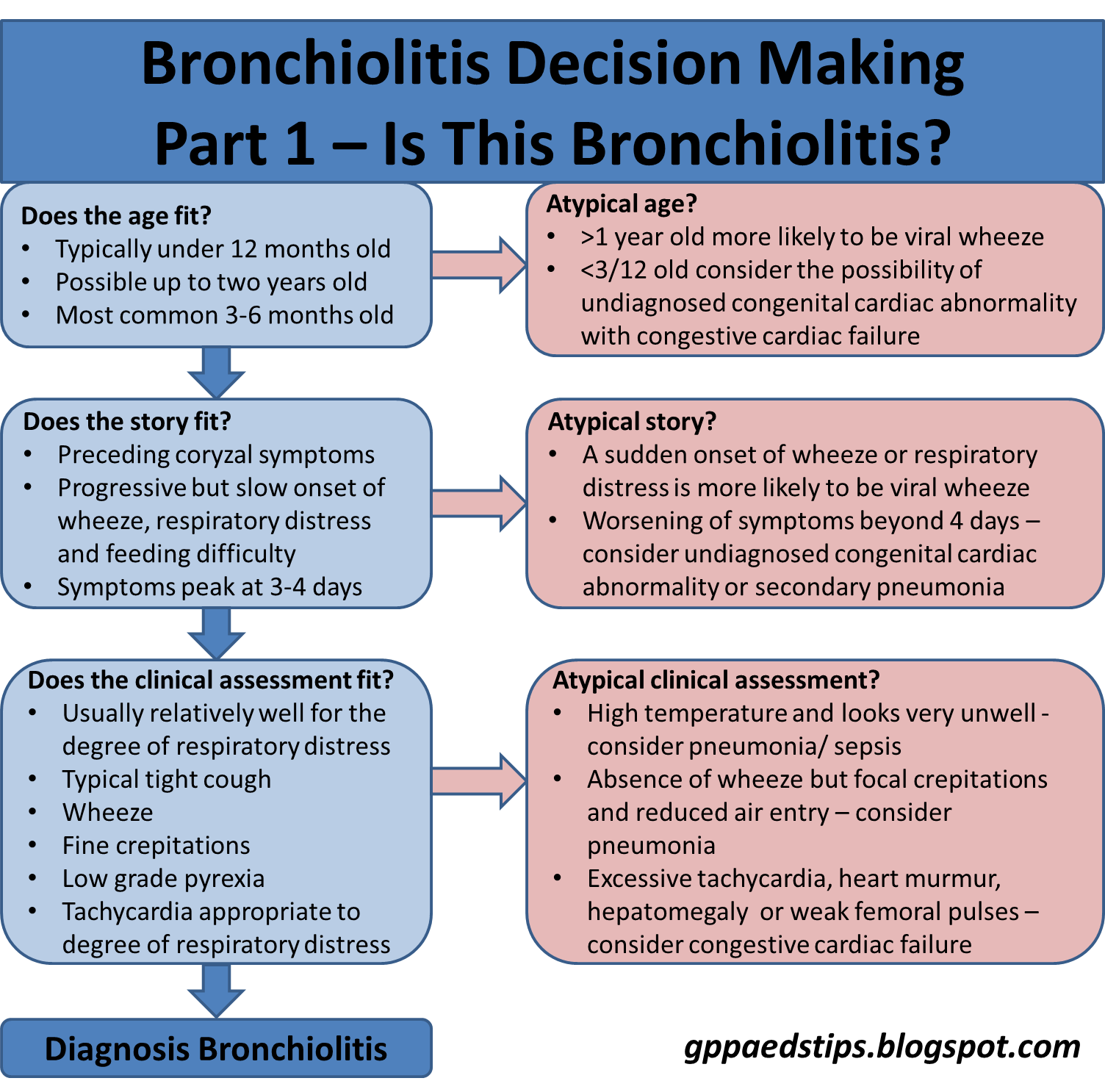
Question 1: Does this child have bronchiolitis?
Most children under the age of 1 year presenting with a tight cough, wheeze, respiratory signs and poor feeding have bronchiolitis. There are other possible explanations for that presentation however and it is important to know about these other possibilities.
Viral induced wheeze, which involves bronchospasm is separate from bronchiolitis. Clues that it may be viral induced wheeze include the age of the child (most commonly over 1 year) and previous episodes of viral induced wheeze. The other clue is the onset of the respiratory changes. Bronchiolitis is a slow accumulation of wetness in the airways and the history is typically of a gradual and progressive worsening of symptoms over days. Viral induced wheeze, due to the bronchospasm involved, presents with a more sudden onset of wheeze and distress, often going from normal to significantly abnormal over a few hours.
Pneumonia is almost never associated with wheeze in children (2). Focal crepitations are often heard in a viral lung infection of any kind. The presence of wheeze strongly suggests that the signs and symptoms are virally induced in some way. Infants with pneumonia will tend to be significantly unwell. The simple rule of thumb is this: If the infant has a wheeze and is well enough to be managed in a pre-hospital setting, they do not have bacterial pneumonia.
Congestive cardiac failure (CCF) due to haemodynamically significant yet undetected congenital cardiac abnormalities is a rare mimic of bronchiolitis but one that is important to be aware of. The typical cause is a large ventricular septal defect (VSD) causing a significant left to right shunt. This increased pressure through the lung circulation causes pulmonary odema which manifests as poor feeding, fine crepitations and wheeze. Thankfully, most significant heart defects are detected before a baby is discharged from postnatal care, but occasionally one slips through and the signs and symptoms are easily mistaken for bronchiolitis.
There are usually clues however. A murmur is the most obvious clue but this can be difficult to hear at >160bpm. An excessive tachycardia is a possible sign of CCF. A significant hepatomegaly (normal babies often have up to a centimetre of palpable liver) is highly suspicious of CCF. Finally, the progression of symptoms does not fit for bronchiolitis as they continue to get worse after the 3-4 days in which bronchiolitis reaches its peak.
Putting these things together, it is usually possible to be confident in diagnosing bronchiolitis as long as the history and findings are consistent with bronchiolitis and not one of the other pretenders.
If the diagnosis is bronchiolitis, we can move onto our next question:
Question 2: Should this child be managed at home or in hospital?
Most children with bronchiolitis can be managed in the community. Keeping people away from hospital where it safe to do so has never been more important. In the UK, the NICE guidelines for bronchiolitis (3) give recommendations for when to refer and when to consider referral.
Referral is always recommended for red flags. In the NICE guidelines, these are a combination of signs of potential respiratory failure. Notably, apnoeas are included as a stand-alone red flag. That means that a child without any chest signs of severe respiratory distress should still be referred if they have had episodes where they appear to stop breathing. The reason for this is that in such cases, immature respiratory drive may be a factor. Following an apnoea, a baby can temporarily seem much improved but may go on to have further events and deteriorate suddenly.
Feeding and hydration is probably the least well defined element of the decision making element. The guidelines ask the clinician to consider a variety of factors, however being able to assess whether the amount of feeding is adequate is next to impossible apart from overt signs of dehydration. We never know how much a breast fed baby is getting unless the answer is "nothing." If the baby is bottle fed, applying a percentage to that as being adequate doesn't take into account the fact that many bottle fed babies take much larger volumes as a baseline. As a result, the most objective measure of adequate feeding has to be signs of hydration or dehydration. For that reason, I have included clinical dehydration in the list of red flags and beyond that, feeding difficulties remain a matter of clinical judgement when it comes to referral.
Possibly the most controversial element of the decision making is the presence of risk factors. In the guidance, it is stated "When deciding whether to refer a child with bronchiolitis to secondary care, take account of any known risk factors for more severe bronchiolitis such as... (e.g.) premature birth, particularly under 32 weeks." The guideline evidence statement lists the basis for each risk factor listed and with the exception of neuromuscular disease, the committee acknowledged that there is no credible published evidence for the other risk factors. Apart from neuromuscular disease, they are all consensus opinion recommendations.
So what are you supposed to do when you see an 8 month old baby with mild bronchiolitis, no red flags and adequate feeding when you know that they were born at 31 weeks gestation? Do you send them to secondary care in case because they have a risk factor for severe bronchiolitis or do you keep them well away from hospital because they don't have severe bronchiolitis and you don't want to add a hospital acquired infection to their list of problems?
Balancing risk vs benefit is what it is all about here. There is a known risk of hospital acquired infection vs an unknown risk of severe bronchiolitis. There is also no evidence that admitting high risk children with bronchiolitis is any safer than good safety-netting advice.
If the decision is made to manage a child with bronchiolitis at home, the third and final question is:
Question 3: What treatment should the child be given?There has been a load of research done to try to find an effective treatment for bronchiolitis. Supportive interventions (oxygen, CPAP etc) in the cases where respiratory support are needed have been shown to be effective. Each and every other therapy have in turn shown to have no benefit for mild to moderate uncomplicated bronchiolitis. Therapies proven to be ineffective include β-agonists, ipratopium, hypertonic saline, antibiotics and corticosteroids. The bottom line is that for a child being managed in the community, no pharmacological treatment should be given. This recommendation is consistent across guidelines from the UK, USA and Australia (3,4,5).
That makes this flowchart nice and simple:
Finally, you might be asking yourself if you are an expert decision maker when it comes to a small person who has a cough and wheeze. Hopefully this post helps you to feel that you are. Decision making in such children is all about recognition, knowing the red flags and above all, learning that if in doubt, looking at the child will almost always give you your answer.
Edward Snelson
@sailordoctor
References
- Roland D, Teo KW, Bandi S, et al COVID-19 is not a driver of clinically significant viral wheeze and asthma Archives of Disease in Childhood Published Online First: 16 October 2020. doi: 10.1136/archdischild-2020-320776
- Hirsch A, Monuteaux M, Neuman M, Bachur R, Estimating Risk of Pneumonia in a Prospective Emergency Department Cohort, Paediatrics, Vol 204, p172-176.E1, Jan 01, 2019 doi:10.1016/j.jpeds.2018.08.077
- Bronchiolitis in children: diagnosis and management, NICE guideline [NG9] Published date: 01 June 2015
- American Academy of Pediatrics Clinical Practice Guideline: The Diagnosis, Management, and Prevention of Bronchiolitis, Pediatrics November 2014, 134 (5) e1474-e1502; doi: 10.1542/peds.2014-2742
- The Royal Children's Hospital Melbourne Clinical Practice Guidelines: Bronchiolitis