One of the things that a crisis should do is to bring people together. As the UK's National Health Service experiences a winter that is bringing it to it's knees, we should be more aware than ever that Primary and Secondary Care need to work together as a team so that we all come out the other end of this intact. There are those in each camp that are so entrenched in the us-and-them mentality that this idea of teamwork is against their very being. If you think that General (family) Practitioners (GPs) are lazy idiots or you think that hospital doctors are arrogant and lack communication skills, I'm not sure that I've got anything to help you. (Perhaps a hug?) If you are willing to believe that we are all part of a team and that any divisions are both understandable and resolvable, read on.
The issues that cause division are (in my experience) usually due to misunderstanding and a lack of insight into the part that we play in creating these disparities. The irritations that I cause my colleagues, whether in Primary or Secondary Care, tend to be completely unintentional. Sometimes it can be what seems like the smallest thing and I have no idea of the impact it has on someone else. That's why it's so important to talk to each other.
Let me describe an example: the seemingly simple act of requesting a chest X-ray for a baby with bronchiolitis.
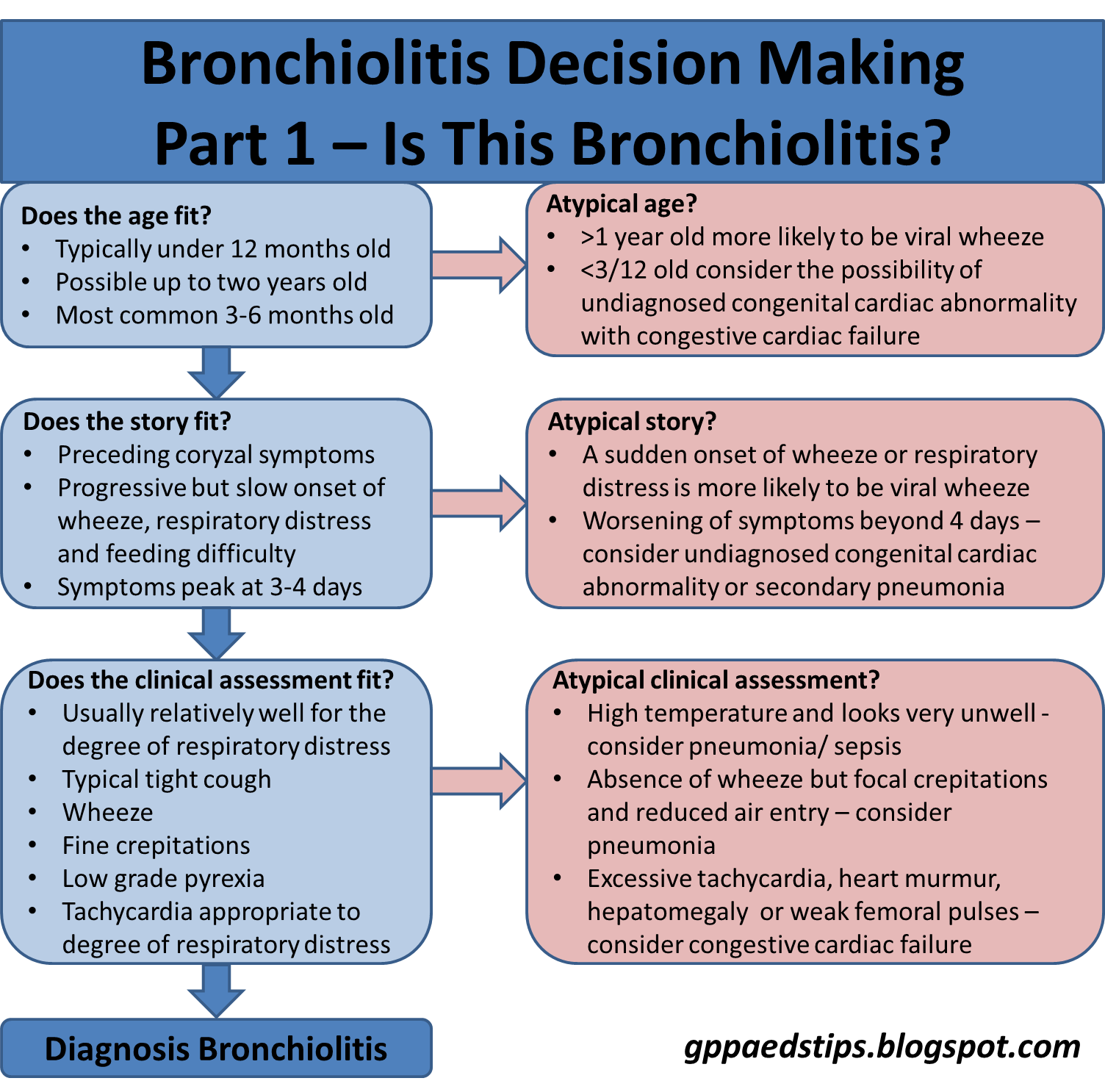
Bronchiolitis is usually a set piece. An infant, usually under 12 months old, gets inflammation in their airways during a viral respiratory tract infection. This leads to a three to five day period of increasing symptoms that usually consist of cough, wheeze, difficulty feeding and increased work of breathing. In practical terms, that might play out like this:
Monday - A three month old is snotty and coughing but well and feeding nicely. Breathing will probably be normal at this stage.
Tuesday - The parents have now noticed some noisy breathing and that feeding isn't as good as it normally is. like many people in these circumstances, they seek a medical opinion and so go to their GP. They are seen and the diagnosis of bronchiolitis is explained. The clinician advises frequent small feeds and gives safety-netting advice for what to look out for in case this child becomes one of the very small minority who develop breathing or feeding difficulties that require support as an inpatient. In keeping with
NICE guidelines (1), they do no tests and give no treatments.
Wednesday - The parents have noticed a slight worsening of the feeding and are unsure about whether this is bad enough to need something to be done. They hold off doing anything during the day but when their baby refuses an evening feed they take their precious bundle to the local emergency department. There the child gets a thorough assessment. Clinically the infant is well hydrated and although they have wheeze and mild recession they are looking happy and have oxygen saturations of 95% in air. Despite the earlier feed refusal, they now take 100 mls of milk. The assessing clinician hears a few crackles in the chest and decides to do a chest X-ray, just to be sure that today's worsening symptoms are not due to a bacterial pneumonia developing.
When is it necessary to do a chest X-ray for babies with bronchiolitis?
There are many possible complications of bronchiolitis. In theory, these should be apparent on a chest X-ray. There are also conditions that mimic simple bronchiolitis, most notably congestive cardiac failure. So, a chest X-ray seems a sensible thing to do to add value to the assessment. Except that it doesn't, for two main reasons.
These are the reasons why a chest X-ray doesn't add value to the assessment of a typical presentation of bronchiolitis:
- There is always something to be seen on the X-ray. If you are looking for normal, you are unlikely to find it.
- If the infant has bronchiolitis, that is enough explanation for their clinical condition. If they had a complication such as lobar pneumonia as well, you would't be doing the chest X-ray to see if there is a problem, you'd be doing it because the child is seriously unwell.

Coming back to our little one with bronchiolitis, let's assume that the chest X-ray shows what it always shows in bronchiolitis - something of uncertain significance. There will be a little fluffy shadow somewhere due to the mucous plugging and atelectasis that is part and parcel of bronchiolitis. Often, there is something to be seen at the right heart border (or as a wise radiologist once redefined for me: "the area of radiological romance") which may or may not be something. Once seen, it is very difficult not to feel the need to treat for possible bacterial infection. This brings me on to the next few reasons for not doing a chest X-ray.
Doing a chest X-ray in bronchiolitis is associated with increased antibiotic prescribing rates. Bacterial superinfection in bronchiolitis is rare and is usually clinically apparent. Bronchiolitis is reason enough to have respiratory symptoms. If a baby also develops pneumonia, they are usually quite unwell and have a marked degree of distress. So, following that logic, for our baby the antibiotics are simply unnecessary, in which case they may do harm. Since one of the problems that comes with bronchiolitis is feeding and hydration, why give these babies a gastric irritant?
Finally, there is a second victim here: the clinician who saw the baby on Tuesday. Despite sterling work by the GP, the parents are likely to believe in retrospect that they were given a poor service.
All the evidence is there:
- The person that they saw in the community did nothing and their child became worse.
- The experts in the hospital did a test which showed that their baby needed antibiotics.
- Antibiotics were given and eventually the bronchiolitis got better.
Why didn't the GP do something when we went the first time?
Of course both clinicians in this story were trying to do their best for the patient. Neither of them had anything on their mind other than trying to ensure the best outcome for the child. There was no disrespect intended and no one wanted to cause anyone any problems. We are all just trying to get through the day and to keep our patients safe and well.
Thankfully, it turns out that in bronchiolitis, keeping your patient safe and well is probably best done without the use of chest x-ray and antibiotics. So, we in Secondary Care can help our colleagues in Primary Care out by making the assessment that needs to be made: in or out (of hospital)? That decision is made on clinical grounds and if they need to be admitted, a chest X-ray may be useful. Maybe.
Edward Snelson
Vice President of the Guild of Doing as Much Nothing as Possible
@sailordoctor
Disclaimer: I did a chest X-ray for bronchiolitis once. There was a white patch at the right heart border but it turned out to be tippex on the screen.
Reference
- Bronchiolitis in children: diagnosis and management, NICE guideline [NG9] Published date: June 2015